Гинекомастия — это доброкачественное увеличение грудных желез или железы у мужчин. Гинекомастия бывает истинная (обусловлена разрастанием железистой ткани - ткани молочной железы), а также ложная (связана с массивными жировыми отложениями при ожирении, которые увеличивают объем грудной железы).
Gynecomastia
Definition
Gynecomastia is enlargement of the male breast due to benign ductal and stromal proliferation so that the breast takes on a female form (Greek gyne, pertaining to women; mastos, breast).
Prevalence and Epidemiology
Approximately 85% of male breast masses are due to gynecomastia, which is the most common disorder in the male breast. It may be detected incidentally at the time of a routine physical examination as either a tender mass beneath the nipple or as a progressive painless enlargement of the breast.[20]
Etiology and Pathophysiology
The development of gynecomastia is believed to be due to hormone imbalance, with a relative excess of female hormones. Pathophysiologic mechanisms resulting in gynecomastia can be divided into the following four categories: (1) estrogen excess; (2) androgen deficiency; (3) androgen receptor defects; and (4) enhanced sensitivity of breast tissue to estrogenic hormones. Gynecomastia can be physiologic or due to underlying diseases, including medication effect. Hormonal manipulation, such as androgen and antiestrogen therapy for prostatic cancer, and drugs, such as digitalis, cimetidine, tricyclic antidepressants, and spironolactone can cause gynecomastia (Table 17-1). Braunstein reported that 25% of patients seeking consultation for gynecomastia are found to have idiopathic gynecomastia; another 25% have pubertal gynecomastia; 10% to 20% of cases are drug related; and 8% are associated with cirrhosis or malnutrition.[21]
TABLE 17-1 -- Conditions Associated with Gynecomastia
Predisposing Conditions
Estrogen excess
Gonadal origin
True hermaphroditism
Testicular estrogen-producing tumors
Nontesticular tumors
Adrenal cortical neoplasm
Lung carcinoma
Hepatocellular carcinoma
Liver disease
Nonalcoholic and alcoholic cirrhosis
Androgen deficiency
Aging
Hypoandrogen states
Primary testicular failure
Klinefelter syndrome (XXY)
Kallmann syndrome
Secondary testicular failure
Trauma
Orchitis
Cryptorchidism
Irradiation
Hydrocele
Varicocele
Spermatocele
Renal failure
Drug-Related Conditions
Drugs with estrogenic or estrogen-related activity
Anabolic steroids
Digitalis
Heroin
Drugs that inhibit the action and/or synthesis of testosterone
Drugs with unknown mechanisms for induction of gynecomastia
Amiodarone
Busulfan
Furosemide
Isoniazid
Methyldopa
Reserpine
Theophylline
Tricyclic antidepressants
Verapamil
Adapted from Bland KI, Page DL. Gynecomastia. In: Bland KI, Copeland EM III, editors. The breast: comprehensive management of benign and malignant diseases. Philadelphia, WB Saunders, 1991.
Manifestations of DiseaseClinical Presentation
Patients with gynecomastia are generally asymptomatic; however, breast tenderness is reported in 20% of cases. If present, nipple discharge should be viewed with suspicion because a much higher percentage of cases of male breast cancer demonstrate this feature compared with cases of gynecomastia. Physiologic gynecomastia has three distinct peaks in age distribution; they are neonatal, pubertal, and senescent.[22]
The physical appearance of the breasts of obese men may simulate gynecomastia through deposition of adipose tissue (pseudogynecomastia).
Imaging Indications and Algorithm
The gold standard for imaging gynecomastia is mammography. If a suspicious mass or calcifications are identified, further imaging may be obtained, including additional mammographic images (spot compression or magnification views) and ultrasonography. There is no role for ultrasound evaluation if the mammogram is diagnostic for gynecomastia in the absence of additional suspicious findings.
Imaging Technique and FindingsMammography
Mammography of the normal breast shows a homogeneously radiolucent appearance with minimal strands of ductal or interlobar connective tissue. The mammographic hallmark of gynecomastia is the presence of a subareolar density concentrically distributed around the nipple.[22] Gynecomastia can be unilateral or bilateral and bilaterally symmetric or asymmetric. Three mammographic patterns of gynecomastia have been described. The first pattern is the early nodular pattern (florid phase on histopathology), which is seen in patients with gynecomastia of less than 1 year's duration.[22] In this type, a relatively well-demarcated mass under the nipple extends into the posterior fatty tissue of the breast in a fan-like configuration, evenly distributed above and below the midplane of the nipple. In more severe cases, the mass becomes triangular in appearance with the nipple at the vertex of the triangle or becomes a subareolar, disc-shaped mass. A later dendritic pattern (quiescent fibrous phase on histopathology) features a flame-shaped central subareolar opacity with prominent linear projections (dendrites) radiating into the deeper adipose tissue toward the upper outer quadrant of the breast. A diffuse glandular pattern features a diffuse, dense nodular parenchyma in an enlarged breast that mimics the density seen in a dense female breast. This pattern of gynecomastia is commonly seen in patients who receive exogenous estrogen, such as men who undergo a sex change operation and those who are treated for advanced prostatic carcinoma. In these situations, the relatively rapid breast enlargement usually has a conical or pyramidal contour, unlike the rather rounded or hemispheric shape found in women. Severe gynecomastia can also be distinguished from a dense female breast by the lack of Cooper ligaments (Figs. 17-26 and 17-27).
FIGURE 17-26Early gynecomastia. Craniocaudal (A) and mediolateral oblique (B) digital mammograms of the left breast in a male patient show glandular tissue in the retroareolar region.
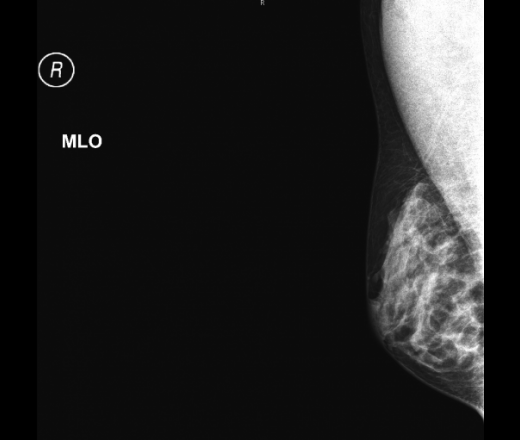
FIGURE 17-27Asymmetric gynecomastia. Bilateral mediolateral oblique (A) and (B) digital mammograms show moderate left gynecomastia and a normal right male breast. A BB denotes a palpable abnormality of the left breast.
Pseudogynecomastia, an enlargement of the breast due to obesity, is readily differentiated from true gynecomastia by means of the preponderance of radiolucent fat and the absence of dense retroareolar tissue in pseudogynecomastia (Fig. 17-28).
FIGURE 17-28Pseudogynecomastia in an obese man. Bilateral mediolateral oblique mammograms (A and B) show only fat, blood vessels, and supporting stroma. The absence of retroareolar densities ruled out true gynecomastia. (From Chantra PK, So GJ, Wollman JS, Bassett LW. Mammography of the male breast. AJR Am J Roentgenol 1995;164:853-858.)
Ultrasonography
The ultrasonographic appearance of gynecomastia demonstrates breast tissue in the subareolar palpable area and often mimics the ultrasonographic findings in developing female breasts.[23] The ultrasonographic appearance of gynecomastia can be directly correlated with the findings on mammographic and histologic examinations. Initially, there is small subareolar hypoechogenicity with a definable, slightly lobulated posterior border representing ductal hyperplasia of the nodular phase. In the dendritic phase, the posterior border of the subareolar hypoechoic change becomes angular with finger-like projections. Occasionally, it may be difficult to differentiate between early carcinoma and nodular gynecomastia because both conditions are hypoechoic. However, changes in gynecomastia are always subareolar in location and the hypoechogenicity is not associated with acoustic shadowing, a finding often seen in carcinoma. In the late stage, when more fibrosis develops, there is an increase in the echogenicity of the breast parenchyma, almost similar to the fibroglandular echogenicity in the female breast (Fig. 17-29).
FIGURE 17-29Gynecomastia. Right breast ultrasound image shows fibroglandular tissue.
Magnetic Resonance Imaging
Gynecomastia appears similar to female normal fibroglandular tissue characterized by homogeneous, non–mass-like enhancement and normal fibroglandulararchitecture. Kinetic analysis shows a slow initial phase and a persistent delayed phase.[24]
Classic Signs
Gynecomastia commonly appears as a flame-shaped central subareolar opacity on a mammogram.
Differential DiagnosisFrom Clinical Presentation
The differential diagnosis for an enlarged breast or palpable mass in the male patient includes gynecomastia, pseudogynecomastia, and breast carcinoma. A complete physical examination should ensue. If clinical findings fail to differentiate among these, imaging is warranted.
From Imaging Findings
The purpose of mammography is to reliably differentiate between benign conditions and breast carcinoma. The differential diagnosis of benign breast conditions in a male breast includes gynecomastia, pseudogynecomastia, lipoma, duct ectasia, intraductal papilloma, fat necrosis, abscess, and epidermal inclusion cyst.




ну чем не женская грудь
Гинекомастия — это доброкачественное увеличение грудных желез или железы у мужчин. Гинекомастия бывает истинная (обусловлена разрастанием железистой ткани - ткани молочной железы), а также ложная (связана с массивными жировыми отложениями при ожирении, которые увеличивают объем грудной железы).
Gynecomastia
Definition
Gynecomastia is enlargement of the male breast due to benign ductal and stromal proliferation so that the breast takes on a female form (Greek gyne, pertaining to women; mastos, breast).
Prevalence and Epidemiology
Approximately 85% of male breast masses are due to gynecomastia, which is the most common disorder in the male breast. It may be detected incidentally at the time of a routine physical examination as either a tender mass beneath the nipple or as a progressive painless enlargement of the breast.[20]
Etiology and Pathophysiology
The development of gynecomastia is believed to be due to hormone imbalance, with a relative excess of female hormones. Pathophysiologic mechanisms resulting in gynecomastia can be divided into the following four categories: (1) estrogen excess; (2) androgen deficiency; (3) androgen receptor defects; and (4) enhanced sensitivity of breast tissue to estrogenic hormones. Gynecomastia can be physiologic or due to underlying diseases, including medication effect. Hormonal manipulation, such as androgen and antiestrogen therapy for prostatic cancer, and drugs, such as digitalis, cimetidine, tricyclic antidepressants, and spironolactone can cause gynecomastia (Table 17-1). Braunstein reported that 25% of patients seeking consultation for gynecomastia are found to have idiopathic gynecomastia; another 25% have pubertal gynecomastia; 10% to 20% of cases are drug related; and 8% are associated with cirrhosis or malnutrition.[21]
TABLE 17-1 -- Conditions Associated with Gynecomastia
Predisposing Conditions
Drug-Related Conditions
Manifestations of DiseaseClinical Presentation
Patients with gynecomastia are generally asymptomatic; however, breast tenderness is reported in 20% of cases. If present, nipple discharge should be viewed with suspicion because a much higher percentage of cases of male breast cancer demonstrate this feature compared with cases of gynecomastia. Physiologic gynecomastia has three distinct peaks in age distribution; they are neonatal, pubertal, and senescent.[22]
The physical appearance of the breasts of obese men may simulate gynecomastia through deposition of adipose tissue (pseudogynecomastia).
Imaging Indications and Algorithm
The gold standard for imaging gynecomastia is mammography. If a suspicious mass or calcifications are identified, further imaging may be obtained, including additional mammographic images (spot compression or magnification views) and ultrasonography. There is no role for ultrasound evaluation if the mammogram is diagnostic for gynecomastia in the absence of additional suspicious findings.
Imaging Technique and FindingsMammography
Mammography of the normal breast shows a homogeneously radiolucent appearance with minimal strands of ductal or interlobar connective tissue. The mammographic hallmark of gynecomastia is the presence of a subareolar density concentrically distributed around the nipple.[22] Gynecomastia can be unilateral or bilateral and bilaterally symmetric or asymmetric. Three mammographic patterns of gynecomastia have been described. The first pattern is the early nodular pattern (florid phase on histopathology), which is seen in patients with gynecomastia of less than 1 year's duration.[22] In this type, a relatively well-demarcated mass under the nipple extends into the posterior fatty tissue of the breast in a fan-like configuration, evenly distributed above and below the midplane of the nipple. In more severe cases, the mass becomes triangular in appearance with the nipple at the vertex of the triangle or becomes a subareolar, disc-shaped mass. A later dendritic pattern (quiescent fibrous phase on histopathology) features a flame-shaped central subareolar opacity with prominent linear projections (dendrites) radiating into the deeper adipose tissue toward the upper outer quadrant of the breast. A diffuse glandular pattern features a diffuse, dense nodular parenchyma in an enlarged breast that mimics the density seen in a dense female breast. This pattern of gynecomastia is commonly seen in patients who receive exogenous estrogen, such as men who undergo a sex change operation and those who are treated for advanced prostatic carcinoma. In these situations, the relatively rapid breast enlargement usually has a conical or pyramidal contour, unlike the rather rounded or hemispheric shape found in women. Severe gynecomastia can also be distinguished from a dense female breast by the lack of Cooper ligaments (Figs. 17-26 and 17-27).
FIGURE 17-26 Early gynecomastia. Craniocaudal (A) and mediolateral oblique (B) digital mammograms of the left breast in a male patient show glandular tissue in the retroareolar region.
FIGURE 17-27 Asymmetric gynecomastia. Bilateral mediolateral oblique (A) and (B) digital mammograms show moderate left gynecomastia and a normal right male breast. A BB denotes a palpable abnormality of the left breast.
Pseudogynecomastia, an enlargement of the breast due to obesity, is readily differentiated from true gynecomastia by means of the preponderance of radiolucent fat and the absence of dense retroareolar tissue in pseudogynecomastia (Fig. 17-28).
FIGURE 17-28 Pseudogynecomastia in an obese man. Bilateral mediolateral oblique mammograms (A and B) show only fat, blood vessels, and supporting stroma. The absence of retroareolar densities ruled out true gynecomastia.
(From Chantra PK, So GJ, Wollman JS, Bassett LW. Mammography of the male breast. AJR Am J Roentgenol 1995;164:853-858.)
Ultrasonography
The ultrasonographic appearance of gynecomastia demonstrates breast tissue in the subareolar palpable area and often mimics the ultrasonographic findings in developing female breasts.[23] The ultrasonographic appearance of gynecomastia can be directly correlated with the findings on mammographic and histologic examinations. Initially, there is small subareolar hypoechogenicity with a definable, slightly lobulated posterior border representing ductal hyperplasia of the nodular phase. In the dendritic phase, the posterior border of the subareolar hypoechoic change becomes angular with finger-like projections. Occasionally, it may be difficult to differentiate between early carcinoma and nodular gynecomastia because both conditions are hypoechoic. However, changes in gynecomastia are always subareolar in location and the hypoechogenicity is not associated with acoustic shadowing, a finding often seen in carcinoma. In the late stage, when more fibrosis develops, there is an increase in the echogenicity of the breast parenchyma, almost similar to the fibroglandular echogenicity in the female breast (Fig. 17-29).
FIGURE 17-29 Gynecomastia. Right breast ultrasound image shows fibroglandular tissue.
Magnetic Resonance Imaging
Gynecomastia appears similar to female normal fibroglandular tissue characterized by homogeneous, non–mass-like enhancement and normal fibroglandulararchitecture. Kinetic analysis shows a slow initial phase and a persistent delayed phase.[24]
Classic Signs
Gynecomastia commonly appears as a flame-shaped central subareolar opacity on a mammogram.
Differential DiagnosisFrom Clinical Presentation
The differential diagnosis for an enlarged breast or palpable mass in the male patient includes gynecomastia, pseudogynecomastia, and breast carcinoma. A complete physical examination should ensue. If clinical findings fail to differentiate among these, imaging is warranted.
From Imaging Findings
The purpose of mammography is to reliably differentiate between benign conditions and breast carcinoma. The differential diagnosis of benign breast conditions in a male breast includes gynecomastia, pseudogynecomastia, lipoma, duct ectasia, intraductal papilloma, fat necrosis, abscess, and epidermal inclusion cyst.
Let me see...
radiographia.ru
Гинекомастия
Let me see...
radiographia.ru
В тему.. Из сегодняшнего (25.03.2013), 1927 г.рождения.
Спасибо за статью.
After the NYear