Девочка, 10 лет. В течение последних трех месяцев лечится в разных больницах по поводу пневмонии.
Девочка из Киргизии. Анамнез жизни без особенностей, из перенесенных заболеваний только гепатит А. Заболела остро в середине июня, отмечался подъем температуры, кашель, слабость. Госпитализирована в стационар в Киргизии, в общем анализе крове - L-8, палочкоядерный сдвиг до 10, СОЭ - 10 мм/ч. На рентгенограмме инфильтративные изменения в S2, 10 справа и околосердечной зоне слева (рентгенограммы не представляю, они безобразного качества). Проведена антибактериальная терапия, клинически состояние с положительной динамикой, рентгенологически тоже положительная динамика слева, справа незначительная положительная динамика. Осмотрена фтизиатром - данных за туберкулез нет, посевы мокроты на ВК отрицательные, реакция Манту отрицательная. Выписана домой. Но дома сохранялся субфебрилитет. Они приехали в наш город (наверное, к родственникам), повторно госпитализирована в детскую больницу в нашем городе. В посевах мокроты - рост Str. pneumoniae и Str. haemolyticus. Повторно назначен курс антибиотиков. КТ картина - это уже после выписки из стационара.
The 4 most common manifestations of Aspergillus lung disease (ie, ABPA, CNPA, aspergilloma, and invasive aspergillosis) have quite different clinical manifestations.
ABPA (acute bronchopulmonary spergillosis) is a syndrome occurring in asthmatic persons and patients with CF that results from a hypersensitivity reaction to Aspergillus colonization of the tracheobronchial tree.
This syndrome may cause fever and pulmonary infiltrates that are unresponsive to antibacterial therapy.
Patients often have a cough and produce mucous plugs, which may form bronchial casts. They may have hemoptysis.
People with asthma who have ABPA may have poorly controlled disease and difficulty tapering off oral corticosteroids.
ABPA may occur in conjunction with allergic fungal sinusitis, with symptoms including chronic sinusitis with purulent sinus drainage.
Aspergilloma (mycetema) may manifest as an asymptomatic radiographic abnormality in a patient with preexisting cavitary lung disease due to sarcoidosis, tuberculosis, or other necrotizing pulmonary processes. Aspergilloma typically develops in the context of preexisting cavitary disease. Aspergillomas may develop in patients with invasive aspergillosis or chronic necrotizing Aspergillus pneumonia.
In patients with HIV disease, aspergilloma may occur in cystic areas resulting from prior Pneumocystis carinii pneumonia.
Of patients with aspergilloma, 40-60% experience hemoptysis, which may be massive and life threatening. Less commonly, aspergilloma may cause cough and fever.
CNPA (chronic necrotizing pulmonary aspergillosis) manifests as a subacute pneumonia unresponsive to antibiotic therapy, which progresses and cavitates over weeks or months.
Patients with CNPA have underlying disease, such as steroid-dependent chronic obstructive pulmonary disease (COPD) or alcoholism, with symptoms that may include fever, cough, night sweats, and weight loss.
Usually, patients have received prolonged courses of antibiotic therapy and sometimes empiric antituberculous therapy without response prior to diagnosis via biopsy or culture.
Invasive aspergillosis typically manifests with fever, cough, dyspnea, pleuritic chest pain, and, sometimes, hemoptysis in patients with prolonged neutropenia or immunosuppression.
For patients at risk for Aspergillus infection after organ transplantation, the most common transplant type at risk is bone marrow. However, invasive aspergillosis may be observed in patients who have received lung, heart, and other solid organ transplants. Of these solid organ transplants, lung transplant recipients are at significant risk. After bone marrow transplantation, invasive aspergillosis has a bimodal distribution, occurring early with prolonged neutropenia before engraftment and later in the context of high-dose corticosteroid therapy for graft versus host disease.
In patients with leukemia and lymphoma, aspergillosis may occur after chemotherapy-induced bone marrow suppression, with resultant prolonged neutropenia, manifesting with persistent fever and pulmonary infiltrates despite broad-spectrum antibiotic therapy. Radiographic and CT scan images may reveal characteristic patterns, including nodules, cavitary infiltrates, and focal infiltrates.
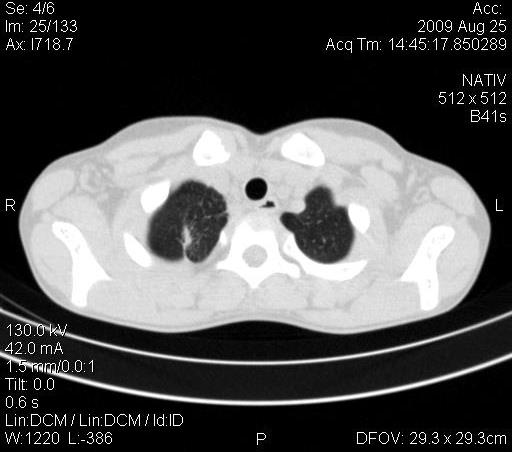

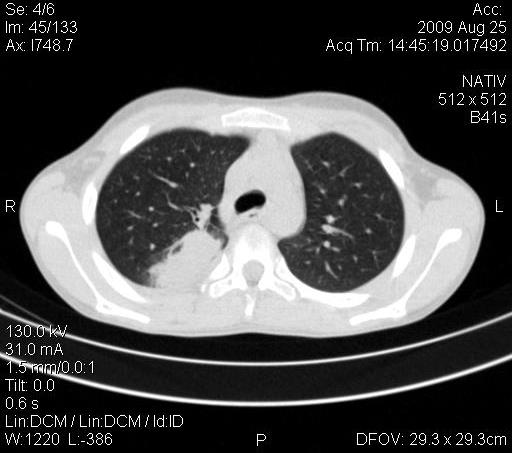






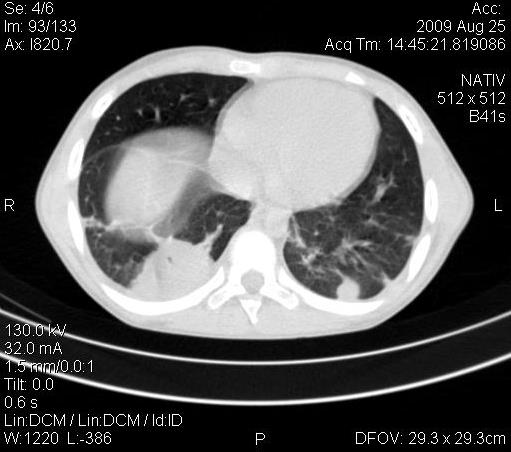



Девочка, 10 лет. В течение последних трех месяцев лечится в разных больницах по поводу пневмонии.
Девочка из Киргизии. Анамнез жизни без особенностей, из перенесенных заболеваний только гепатит А. Заболела остро в середине июня, отмечался подъем температуры, кашель, слабость. Госпитализирована в стационар в Киргизии, в общем анализе крове - L-8, палочкоядерный сдвиг до 10, СОЭ - 10 мм/ч. На рентгенограмме инфильтративные изменения в S2, 10 справа и околосердечной зоне слева (рентгенограммы не представляю, они безобразного качества). Проведена антибактериальная терапия, клинически состояние с положительной динамикой, рентгенологически тоже положительная динамика слева, справа незначительная положительная динамика. Осмотрена фтизиатром - данных за туберкулез нет, посевы мокроты на ВК отрицательные, реакция Манту отрицательная. Выписана домой. Но дома сохранялся субфебрилитет. Они приехали в наш город (наверное, к родственникам), повторно госпитализирована в детскую больницу в нашем городе. В посевах мокроты - рост Str. pneumoniae и Str. haemolyticus. Повторно назначен курс антибиотиков. КТ картина - это уже после выписки из стационара.
АСПЕРГИЛЛЁЗ.
Последняя рентгенограмма.
The 4 most common manifestations of Aspergillus lung disease (ie, ABPA, CNPA, aspergilloma, and invasive aspergillosis) have quite different clinical manifestations.
ABPA (acute bronchopulmonary spergillosis) is a syndrome occurring in asthmatic persons and patients with CF that results from a hypersensitivity reaction to Aspergillus colonization of the tracheobronchial tree.
This syndrome may cause fever and pulmonary infiltrates that are unresponsive to antibacterial therapy.
Patients often have a cough and produce mucous plugs, which may form bronchial casts. They may have hemoptysis.
People with asthma who have ABPA may have poorly controlled disease and difficulty tapering off oral corticosteroids.
ABPA may occur in conjunction with allergic fungal sinusitis, with symptoms including chronic sinusitis with purulent sinus drainage.
Aspergilloma (mycetema) may manifest as an asymptomatic radiographic abnormality in a patient with preexisting cavitary lung disease due to sarcoidosis, tuberculosis, or other necrotizing pulmonary processes. Aspergilloma typically develops in the context of preexisting cavitary disease. Aspergillomas may develop in patients with invasive aspergillosis or chronic necrotizing Aspergillus pneumonia.
In patients with HIV disease, aspergilloma may occur in cystic areas resulting from prior Pneumocystis carinii pneumonia.
Of patients with aspergilloma, 40-60% experience hemoptysis, which may be massive and life threatening. Less commonly, aspergilloma may cause cough and fever.
CNPA (chronic necrotizing pulmonary aspergillosis) manifests as a subacute pneumonia unresponsive to antibiotic therapy, which progresses and cavitates over weeks or months.
Patients with CNPA have underlying disease, such as steroid-dependent chronic obstructive pulmonary disease (COPD) or alcoholism, with symptoms that may include fever, cough, night sweats, and weight loss.
Usually, patients have received prolonged courses of antibiotic therapy and sometimes empiric antituberculous therapy without response prior to diagnosis via biopsy or culture.
Invasive aspergillosis typically manifests with fever, cough, dyspnea, pleuritic chest pain, and, sometimes, hemoptysis in patients with prolonged neutropenia or immunosuppression.
For patients at risk for Aspergillus infection after organ transplantation, the most common transplant type at risk is bone marrow. However, invasive aspergillosis may be observed in patients who have received lung, heart, and other solid organ transplants. Of these solid organ transplants, lung transplant recipients are at significant risk. After bone marrow transplantation, invasive aspergillosis has a bimodal distribution, occurring early with prolonged neutropenia before engraftment and later in the context of high-dose corticosteroid therapy for graft versus host disease.
In patients with leukemia and lymphoma, aspergillosis may occur after chemotherapy-induced bone marrow suppression, with resultant prolonged neutropenia, manifesting with persistent fever and pulmonary infiltrates despite broad-spectrum antibiotic therapy. Radiographic and CT scan images may reveal characteristic patterns, including nodules, cavitary infiltrates, and focal infiltrates.
Какие будут мнения?
А, почему молчание уважаемые коллеги?
Что, Вы часто "такое" зрите?
Двусторонняя нижнедолевая пневмония. Справа абсцедирующая, слева- не уверен. Стопудово не скажу по фотографиям.
Классика жанра..., рядом Сергей, рядом, но не в цель...
Аспергилез?
+1
Симптом "погремушки" (полумесяца) в наличии.
От терапевта.
Могу предположить, что осумкованный адгезивный плеврит справа. Хотя ндо смотреть по клинике. Может и эмпиема быть.