Селшук Пекер, Х. Ибрахим Сан, Сердар Озген, Озлем Курткайя, М. Некметтин Памир
Институт неврологических наук Мармарского университета, Стамбул, Турция
Sinus Pericranii, хирургия, сосудистая патология.
Sinus Pericranii - флюктуирующая сосудистая опухоль с четкими границами, расположенная под кожей черепа. Она сообщается непосредственно с внутричерепной венозной системой. Данный вид патологии наиболее характерен для детской возрастной группы.
По мнению Marras [5], первое упоминание о развитии подобного состояния вследствие перелома костей черепа приходится на 1760 год и, вероятно, связано с именем Percivall Pott. В 1845 Hecker вводит новый термин для обозначения данного феномена: "varix spurius circumscriptus venae diploicae frontalis" [2].
В данном сообщении мы приводим описание Sinus Pericranii у молодого человека.
Описание случая
Молодой мужчина (21 год) поступил с жалобами на головную боль и припухлость мягких тканей в правой лобной области, которые наблюдались в течение года. Kакие-либо сведения о травме головы в анамнезе отсутствовали.
При клиническом осмотре было обнаружено мягкое, податливое и не пульсирующее объемное образование в правой лобной области размером 5´3 см. Состояние кожных покровов над ним было в норме. Размер образования увеличивался при выполнении пациентом движения согласно тесту Valsalva. Неврологическое обследование не выявило каких-либо патологических изменений.
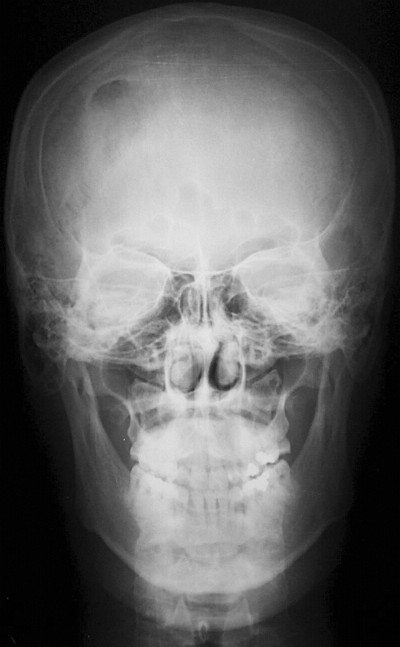
Обзорные рентгеновские снимки черепа свидетельствовали о наличии участка остеолизиса со склеротическими краями в правой лобной области (рис.1).
Рис.1. Обзорная рентгенограмма черепа: область остеолизиса лобной кости справа.
По данным компьютерной томографии (КТ) на поверхности лобной кости отмечалась небольшая эрозия (рис.2).
Рис.2. КТ в режиме костного окна свидетельствует о наличии эрозии на поверхности кости.
Обследование с помощью магнитно-резонансной томографии (МРТ) выявило наличие образования, которое было гипо- и гиперинтенсивным на Т1- и Т2-взвешенных изображениях соответственно. При использовании Gd-DTPA оно характеризовалось неоднородным усилением (рис.3).
Рис.3. Сагиттальное Т1-взвешенное изображение с усилением Gd-DTPA.
Был поставлен следующий клинический диагноз: Sinus Pericranii.


Хирургическое лечение
Под общим наркозом был выполнен дугообразный разрез кожи выше линии волос. Опухоль располагалась под надкостницей.



Выявленная патология. По данным микроскопического исследования опухоль состояла из множества венозных сосудов с отсутствующим мышечным слоем, выстланных обычными эндотелиальными клетками. В ряде областей внутри опухоли была обнаружена фиброзная ткань.
Обсуждение
Sinus Pericranii - это скопление венозных сосудов без мышечного слоя или венозная гемангиома, плотно прилегающая к наружной поверхности кости черепа и сообщающаяся внутри черепа непосредственно с синусом твердой мозговой оболочки через диплоические вены [2].
В 1850 г. Stromeyer описал этот вид патологии, как "субпериостальную кисту черепа, заполненную кровью и сообщающуюся с синусом твердой мозговой оболочки", и предложил термин Sinus Pericranii [8]. Медицинская литература содержит множество терминов для обозначения данной нозологической единицы: простое варикозное расширение (varix simplex), гроздевидное варикозное расширение (varix racemosus), варикозный герниоз (varix herniosis), варикозная аневризма (cirsoid aneurysm), венозная ангиома (venous angioma), варикозно расширенная вена (varix cirsoideus), остеососудистый свищ (fistule osteovasculaire), венозная опухоль костей черепа, варикоз вен черепа [7].
Причина появления этого образования пока не ясна. Обычно Sinus Pericranii считается врожденной патологией, хотя есть предположения, что травма также может быть возможным причинным фактором, по крайней мере, в ряде случаев [4]. Общепринятым критерием для установления первопричины данной патологии является тип ткани, выстилающей мешок. Эндотелиальная выстилка характерна для врожденного Sinus Pericranii, тогда как приобретенное образование имеет выстилку из соединительной ткани [7]. Микроскопическое исследование опухоли в нашем случае свидетельствовало о наличии эндотелиальных клеток. Таким образом, мы пришли к выводу о врожденном характере Sinus Pericranii у нашего больного.
Обычно Sinus Pericranii располагается по соседству с синусами твердой мозговой оболочки. Есть несколько сообщений о его латеральной локализации в лобной или лобно-височной областях [7].
Как правило, эта патология не проявляется какими-либо симптомами. Характерной чертой данного образования является увеличение его размера при повышении внутричерепного давления, обусловленного плачем, выполнением движения согласно тесту Valsalva или вынужденным положением [1]. Размер опухоли уменьшается при непосредственном надавливании или подъеме головы. Это патологическое состояние может развиться в любом возрасте. Однако большинство пациентов обычно моложе 30 лет. Соотношение между больными мужского и женского пола составляет 2:1 [1].
Клинический диагноз Sinus Pericranii может быть поставлен на основании появления мягкого флюктуирующего образования, локализующегося возле синуса твердой мозговой оболочки и увеличивающегося в размере при выполнении движения в соответствии с тестом Valsalva [2]. Данные обзорного рентгенографического исследования могут свидетельствовать о наличии гипоплотной области, расположенной ниже опухоли. КТ с использованием костных окон позволит выявить четко выраженное остеолитическое поражение. Что касается нашего больного, то данные КТ исследования указывали на наличие небольшой эрозии на поверхности лобной кости. Кроме того, может быть виден отек мягких тканей. МРТ дает информацию о содержимом синуса на основании характеристик сигнала и взаимосвязи между поражением и подлежащим синусом [4]. Sadler [6] описал больного, обследованного с помощью МРТ, данные которой указывали на поражение, характеризующееся сигналом со смешанной интенсивностью. Это было обусловлено турбулентным кровотоком. Для определения взаимосвязи между образованием и синусами твердой мозговой оболочки можно применять МР-венографию [1].
Несмотря на данные о возможном спонтанном регрессе Sinus Pericranii [2], в целом, он имеет тенденцию к постепенному росту [7]. У большинства больных какие-либо симптомы отсутствуют. Таким образом, основной целью хирургического лечения является устранение косметического дефекта. Кроме того, удаление образования позволит предотвратить сильное кровотечение и возможность травматической воздушной эмболии. Хирургическое лечение заключается в простом удалении опухоли и блокировании или подавлении коммуникантных вен. У нашего больного коммуникантные диплоические вены были заблокированы с помощью костного воска. Ряд авторов сообщает о применении обширной краниотомии или краниоэктомии в целях удаления данной мальформации [5]. В литературе не описаны случаи, когда окклюзия этого патологического пути привела к развитию внутричерепной венозной гипертензии [3]. К возможным осложнениям данного хирургического вмешательства относятся воздушная эмболия и кровотечение.
ЛИТЕРАТУРА
- Azusawa H., Ozaki Y., Shindoh N., Sumi Y. Usefulness of MR venography in diagnosis sinus pericranii: Case report. // Radiation Medicine. - 2000. - Vol.18 (4). - P. 249-252.
- Bollar A., Allut A.G., Prieto A., Gelabert M., Becerra E. Sinus pericranii: radiological and etiopathological considerations. // J. Neurosurg. - 1992. - Sept. - Vol. 77. - P. 469-72.
- Desai K., Bhayani R., Goel A., Muzumdar D. Sinus pericranii in the frontal region: A case report. // Neurology India. - 2001. - Sept. - Vol. 49. - P. 305-7.
- Jung S., Lee J.K., Kim S.H., Kim J.H., Kang S.S., Lee J.H. Parietal sinus pericranii. // Surg. Neurol. - 2000. Sept. Vol. 54(3). - P. 270-3.
- Marras C., McEvoy A.W., Grieve J.P., Jager H.R., Kitchen N.G., Villani R.M. Giant temporooccipital sinus pericranii: A case report. // J. Neurosurg. Sci. - 2001. - Jun. - Vol. 45(2). P. 103-6.
- Sadler L.R., Tarr R.W., Jungreis C.A. Sinus pericranii: CT and MR findings. // J. Comput. Assist. Tomogr. - 1990. Vol. 14. - P. 124-7.
- Spektor S., Weinberger G., Constantini S., Gomori J.M., Beni-Adani L. Giant lateral sinus pericranii. // J. Neurosurg. - 1998. - Jan. - Vol. 88. - P.145-7.
- Stromeyer L. Ueber Sinus pericranii. .// Dtsch. Klin. - 1850. - Vol. 2. - P. 160-1.
Sinus Pericranii
Sinus Pericranii
http://www.ajnr.org/content/25/1/121.full
Sinus Pericranii
http://www.pediatricneurosciences.com/article.asp?issn=1817-1745;year=2010;volume=5;issue=1;spage=39;epage=41;aulast=Kamble
"Таким образом, основной целью хирургического лечения является устранение косметического дефекта."
Два случая лично- никто и не пытался оперировать. Достаточно разъяснения патологии больному.
Идиопатический внутричерепной гиперостоз
Nosotros pensamos que el fenómeno de hiperostosis tiene una función protectora del tejido cerebral. Envuelve al parenquima encefálico con suma delicadeza, en aquellas pacientes mayores de 65 años que sufren atrofia cerebral importante. Con eso el encéfalo queda como protegido en un estuche entre algodones. Nunca se han encontrado lesiones cerebrales en las necropsias de pacientes con hiperostosis frontal interna. La disminución de los espacios libres intracraneales evita que los movimientos bruscos, como un simple traspiés, puedan provocar elongación de las venas y desencadenar una hemorragia. A lo largo de los años hemos comprobado que las mujeres mayores, con hipersostosis craneal, no sufren hematomas subdurales, como los varones. Por el contrario las mujeres mayores que no padecen atrofia cerebral, tampoco llegan a desarrollar Hiperostosis Craneal. Este hallazgo demuestra que la causa que desencadena la hiperostosis sería la atrofia cerebral que pondría en marcha el proceso de osteogénesis intracraneal. Este fenoméno ya está descrito en los niños con hidrocefalia congénita que luego se corrige quirúrgicamente.
.
Osteogenesis:
Según la superficie craneal que abarca la Hiperostosis se distinguen dos tipos bien diferenciados
A) HIPEROSTOSIS FRONTAL INTERNA: La hiperostosis frontal interna se caracteriza por un engrosamiento del díploe del hueso frontal que hace prominencia en la cavidad craneal. No se extiende más allá de la sutura coronal (flechas). Es la forma más común y se considera una variante anatómica normal.
FIGURA 2) Hiperostosis frontal interna típica que afecta exclusivamente al hueso frontal. (Typical frontal hyperostosis that exclusively involves frontal bone).
FIGURA 3) Ventana de Hueso: Hiperostosis frontal interna típica que afecta exclusivamente al hueso frontal. (Bone Window: Typical frontal hyperostosis that exclusively involves frontal bone).
FIGURA 9) Con ventana de hueso se puede apreciar el engrosamiento del díploe y el contorno mamelonado de la tabla interna del craneo, hallazgos característicos de Hiperostosis Craneal Difusa Idiopática.
(Image manipulated with Windows PAINT program. In the previous image has been painted a strip of bone that simulates an internal frontal hyperostosis. No doubt the brain parenchyma is more subject and the possibility of breaking a vein by a sudden acceleration process is more difficult.)
1) HIPEROSTOSIS CRANEAL DIFUSA.
94 years old, female. She consulted by headaches.
FIGURA 3)
FIGURA 5)
Cisterna Magna
FIGURA 2) Vista de la Cisterna Magna en proyección coronal.
(View of the Cisterna Magna in coronal projection)
CASO 1
CASO 2
CASO 3
CASO 4
(View of the Megacisterna Magna in this MRI axial image. The existence of meningeal septa, and the lateral extensions in form of wings, enables us to distinguish it from an arachnoid cyst)
CASO 5
(Megacisterna Magna in this MRI axial image. The existence of meningeal septa, and the lateral extensions in form of wings, enables us to distinguish it from an arachnoid cyst)
FIGURA 3) Megacisterna Magna en una imagen de TC axial.
(Megacisterna Magna in this CT axial image.)
CASO 6
(Megacisterna Magna in this MRI axial image. Vermian Atrophy)
CASO 7
(Megacisterna Magna in this MRI axial image. Cerebellar atrophy. The falx cerebelli)
CASO 8
FIGURA 1) Proyección sagital de una Megacisterna Magna. Atrofia vermiana.
(Sagittal projection of a Megacisterna Magna. Vermian atrophy. )
(Megacisterna Magna in this MRI axial image. Cerebellar atrophy. Falx cerebelli)
CASO 9
(Megacisterna Magna in this MRI axial image. Falx cerebelli. Cerebellar atrophy)
CASO 10
(Megacisterna Magna in this CT axial image. )
(Megacisterna Magna in this CT axial image. Falx cerebelli )
CASO 11
(Megacisterna Magna in this CT axial image. Meningeal septa. Cerebellar atrophy.)
FIGURA 2) Megacisterna Magna. Septos meningeos. Atrofia cerebelosa
(Megacisterna Magna. Meningeal septa. Cerebellar atrophy.)
(Posteroanterior perspective of the external occipital protuberance. Toshiba Aquilion 64 CT Scanner).
(And another slice, still more caudal)
MÁS IMÁGENES........................MORE IMAGES
CASO 1)
FIGURA 1)
FIGURA 2)
CASO 2
FIGURA 2) El espolón contiene hueso compacto cortical y hueso esponjoso.
(The spur contains compact bone cortical and cancellous bone).
Hospital Universitario Miguel Servet. (HUMS) Zaragoza.Spaiñ