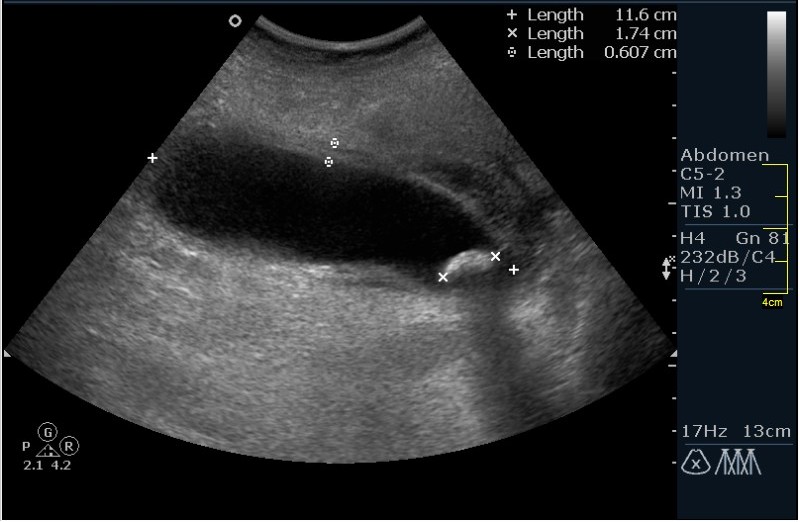
Пузырь напряжен, стенка слоистая, рыхлая, отек паравезикальной клетчатки, в ложе пузыря прослойка выпота, в шейке вклиненный камень(хотя так утверждать нельзя т.к. в публикации не указаны сканы со сменой положения тела.). ЖКБ. Острый обтурационный холецистит.
US features: * Luminal distention > 4 cm (width) * Wall thickening > 5 mm (edema, congestion); thickening is usually worse on the hepatic side * Gallstones; CD stones may be difficult to detect if they are not surrounded by bile * Positive Murphy's sign (sensitivity, 60% specificity 74%),
* Pericholecystic fluid
* Pain: Murphy's sign
Complications:
* Gangrenous cholecystitis: rupture of GB; mortality 20%, gangrene causes nerve death so that 65% of patients have a negative Murphy's sign * Emphysematous cholecystitis, rare (40°h occur in diabetics)
* Empyema
CHRONIC CHOLECYSTITIS:
US features: * GB wall thickening (fibrosis, chronic inflammation) * Intramural epithelial crypts (Rokitansky-Aschoff sinuses) * Gallstones, 95% Failure of GB to contract in response to CCK
US features: No calculi Sludge and debris Usually in critically ill patients Same findings as in calculous cholecystitis: Sonographic Murphy's sign, GB wall thickening (> 2 mrn), Pericholecystic fluid. But may occur in abscence of any of the above findings HIDA scanning (radionuclear scan) Nonvisualization of GB
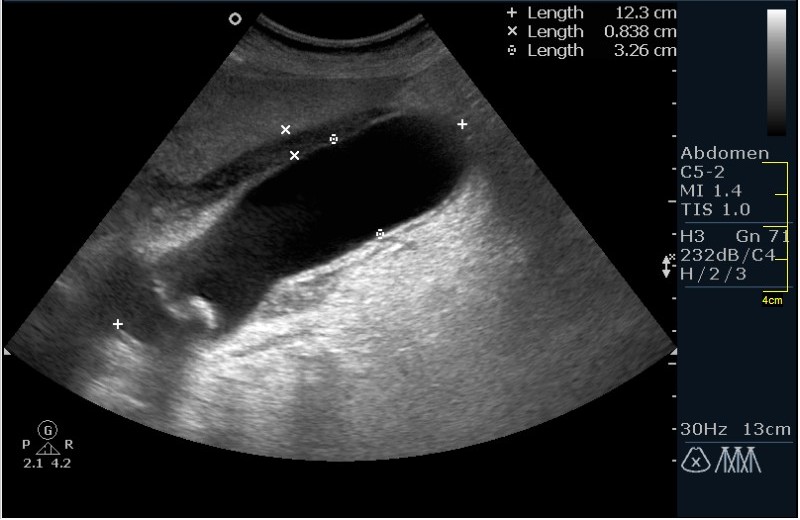

Пузырь напряжен, стенка слоистая, рыхлая, отек паравезикальной клетчатки, в ложе пузыря прослойка выпота, в шейке вклиненный камень(хотя так утверждать нельзя т.к. в публикации не указаны сканы со сменой положения тела.). ЖКБ. Острый обтурационный холецистит.
Марио как Вы классифицируете холециститы.
Cholecytithis:
ACUTE CHOLECYSTITIS
Causes:
Gallstone obstruction, 95%
Acalculous cholecystitis, 5%
US features:
* Luminal distention > 4 cm (width)
* Wall thickening > 5 mm (edema, congestion); thickening is usually worse on the hepatic side
* Gallstones; CD stones may be difficult to detect if they are not surrounded by bile
* Positive Murphy's sign (sensitivity, 60% specificity 74%),
* Pericholecystic fluid
* Pain: Murphy's sign
Complications:
* Gangrenous cholecystitis: rupture of GB; mortality 20%, gangrene causes nerve death so that 65% of patients have a negative Murphy's sign
* Emphysematous cholecystitis, rare (40°h occur in diabetics)
* Empyema
CHRONIC CHOLECYSTITIS:
US features:
* GB wall thickening (fibrosis, chronic inflammation)
* Intramural epithelial crypts (Rokitansky-Aschoff sinuses)
* Gallstones, 95%
Failure of GB to contract in response to CCK
ACALCULOUS CHOLECYSTITIS:
Clinical settings associated with acalculous cholecystitis:
* Trauma
* Burn patient
* Prolonged fasting (postoperative patients), hyperalimentation
* Diabetes
* AIDS
* Others: colitis, hepatic arterial chemotherapy, postpartum, vascular insufficiency
US features:
No calculi
Sludge and debris
Usually in critically ill patients
Same findings as in calculous cholecystitis: Sonographic Murphy's sign, GB wall thickening (> 2 mrn), Pericholecystic fluid. But may occur in abscence of any of the above findings
HIDA scanning (radionuclear scan)
Nonvisualization of GB
Let me see...
radiographia.ru
Спасибо, взял на заметку.!